
“The two low points of my cancer treatment were the day I was diagnosed and the day the hospital updated their electronic medical record system,” says Dr. Mary L. Witkowski, who underwent treatment for Hodgkin’s lymphoma in her final year of medical school. At the time, she had four young children. Diagnosis day stands out for good reason, but the day that the new electronic medical record system arrived at the hospital may seem a bit odd. However, the rollout was so cumbersome that it stalled patient care. “The system was to be built using clinician input. But it was still taking them 20 times longer to do any procedure,” she says. Rather than the typical three-hour stay, Witkowski stayed for 12 hours going from bloodwork to vitals to chemotherapy. “The worst part was waiting for the chemotherapy,” she said. “When you’re getting chemotherapy, it’s like you’re waiting for a punch. You know it is killing the cancer, but you’re going to feel horrible pretty soon.” She goes on, “I just sat there waiting for the drugs, waiting for the punch, never knowing when it would hit. But every step in the care chain, like laboratory services and pharmacy, is backed up and doesn’t have the right data and information on your treatment. You see firsthand the complexity and interdependence of the delivery system, which directly impacts the patient.”
In health informatics, the gathering, measuring, and assessing of patient data is a critical component of overall care.
Witkowski, who is now a senior fellow at Harvard Business School researching the strategy and equity of health care delivery, has been cancer-free for years. Since her diagnosis, electronic medical records (EMR, or sometimes EHR for electronic health records) have come a long way; still, the promise they hold—first, of making care more efficient and then of broadening access to information and tracking critical outcomes—is still being fully realized. Indeed, the EMR industry was valued at $29 billion in 2020 and is expected to reach $38.4 billion by 2026. Provisions from the Affordable Care Act, in particular, incentivized hospitals to embrace digital innovation, making the field into the burgeoning industry it is now.
In many ways, the core purpose behind EMR is to provide an easy, secure, and accessible forum to transmit information between different health care providers and patients. Underlying all of this is the importance of what is often called health informatics, where the gathering, measuring, and assessing of patient data is a critical component of overall care.
Depending on one’s framing, how one’s medical team deals with your health data can lead to quality care and/or an increased administrative burden. What does this tell us about the legal informatics field? How do you balance the “burden” with creating quality outcomes? And where can technology step in to increase efficiency, and not simply add bloat to the system?
In this story, we explore the idea of health informatics through the work of Witkowski, who conducts research at the Institute for Strategy and Competitiveness (ISC) at Harvard Business School (HBS) with Professor Michael Porter. Witkowski, who obtained an MBA from HBS prior to receiving her medical degree and worked at Bain in management consulting, is an expert on the relationship between quality metrics in the health care field and better health outcomes. She is also an evangelist for developing better standards in medicine, which, she says, has to start with the reason for being in the business of health from the start—making patients better.
Measuring value
Outcomes measurement is an important aspect of ISC’s research focus into value-based health care. “Wherever we see systematic measurement of results in health care—no matter what the country—we see those results improve,” wrote Porter and Thomas E. Lee in Harvard Business Review in 2010. ISC is broadly tasked with research on competition (for example, between entities like nations and companies). As part of this, it has a strong interest in “creating shared value,” or the idea that strategy might create both corporate profit and social good. This idea feeds into Witkowski’s health care research at ISC.
“A lot of people hear value-based health care, and they make analogies to Kmart,” says Witkowski. “But I think of value as the results that matter to patients. There’s so much value in the patient–clinician connection. But the health care delivery system does everything it can to destroy that value.”
How do you define “quality” in health care? And critically, what are the measurements of quality—the standards—we’re taking to assess these outcomes?
In value-based health care, scholars are interested in redesigning health care delivery on a systemic level. This means asking what outcomes matter to patients and working outward: What technology is needed to support this? How should we train doctors to support this? How do you define “quality” in health care? And critically, what are the measurements of quality—the standards—we’re taking to assess these outcomes?
As Witkowski notes, deciding what to measure—and how—has been tricky for health care, where even viewing it as a business with economic implications moves into thorny territory.
Health care has been open to, as she puts it, “structural measures” like, “Is my facility to code? Has it been licensed? Do my nurses and doctors have the right degrees?” (In much the same way, law often turns to similar input-based metrics, such as where one went to law school or how many offices the firm has globally as a proxy for a more outcome-based understanding on quality.)
We have had a lot of pushback on the answer to: Are we doing a good job or not for patients?
Dr. Mary Witkowski
Then, Witkowski says, health care moved to studying process: “People felt comfortable measuring what they do,” she says. As a case in point, safety checklists have now become commonplace throughout the industry as a means of improving overall outcomes for the patient physically, but also reducing downstream complications that could put additional burdens on the system. (Again, there are striking parallels to what is occurring in law vis-à-vis the advent and rise of legal operations departments and their attempts to improve process flows and other activities.)
But, Witkowski says, health informatics has only just begun to deal with what, from her point of view, is perhaps the most important measure of all—assessing the overall results of care, namely the health outcomes that matter to patients. “We have had a lot of pushback on the answer to: Are we doing a good job or not for patients? In any field, nobody likes to be measured and held accountable for that. That’s the real challenge, and that’s the real opportunity.” (In law, the development of input-based metrics is an important component of assessing the overall quality of legal services.)
Indeed, underscoring the importance of patients in this debate, to understand what to measure, how, and where that data goes, Witkowski looks to patients before she looks at IT. “Health care is largely a knowledge business,” she says. “First and foremost, what is the information we want to capture from the patients? How are we obtaining that content and investing in structures that help us create value for the patients?” She goes on:
You have to really listen to the patient to understand what’s going on and compare that to the information that’s available. You then have to put in time in communicating back to the patient and the delivery team. The physician’s role in health care is about both deciding what is the problem and how are we going to treat it? Then, what should the plan be in communicating that? A lot of times people think of the informatics as, ‘Oh, we’re doing all these things and then we have to think about IT.’ I feel that health care really needs to be thought of as an information business to start with. We’ve done a terrible job in this area.
Technology does have a role, however—but it needs to be built with patients and doctors in mind. “Day-to-day, the questions that come up are: Are our information systems built for the way in which we’re practicing health care? Are they built for teams, and are they interoperable?” says Witkowski. For now, the answer is no.
In fact, one of the major challenges associated with EMR has been interoperability: Can the systems talk to each other? Similarly, are the systems—and more gradually, the electronic records—built to store and disseminate information with outcomes measurement in mind?
The PROVE Center at Brigham and Women’s Hospital and Dr. Andrea Pusic are aiming to make change in this area. In addition to a variety of projects that aim to gather and utilize patient outcomes across medical procedures and diseases, Dr. Pusic has also created a platform that can work on top of some of the more popular health record information systems to gather the kinds of outcomes ISC is in favor of aggregating and standardizing. Dr. Pusic has not only helped pave the way for the digital infrastructure that could improve the system, but according to Witkowski, she should also be recognized for her attention to posing questions like: How do we ask the right questions to obtain the right information and then give the right information back to patients in a way that’s meaningful? How do we gather the right measures to clinically improve our care?”
Dr. Pusic does what Witkowski hopes the whole system would do. Start with the patient—and the need to create value for the patient—and build the system from there.
Standards of care
Witkowski breaks down the relationship between health informatics and value-based health care into four buckets.
- How do we engage with patients and get the information to even be having the right conversation?
- How are we using that information in care delivery?
- How do we determine and measure the results that matter most to patients?
- How do we ensure we are communicating with all patients and technology that is accessible regardless of race or language spoken?
In 2012, ISC, Boston Consulting Group, and the Karolinska Institute spun out a nonprofit to deal with this third question: the International Consortium for Health Outcomes Measurement (ICHOM), whose mission is drive value-based health care by “defining global Standard Sets of outcome measures that matter most to patients and driving adoption and reporting of these measures worldwide to create better value for all stakeholders.”
Measuring outcomes at ISC means defining value—a tricky equation (see figure 1). As Witkowski’s research makes clear, the current health care landscape does not reward quality on a costing basis. A poor outcome might result in further ER visits, which might result in additional tests and costs. What would it look like to measure outcomes on a long-term basis? (For more on the economic and organizational angle on medicine and law, see an interview with Leemore Dafny, Bruce V. Rauner Professor of Business Administration at Harvard Business School, in “Canary in a Coal Mine? What legal services can learn from health care’s consolidation experience.”)
A host of acronyms—or reporting mechanisms—have sprung up to fill this gap. There are patient-reported outcome measures (PROMs), clinically reported outcomes (CROs), and patient-reported experience measures (PREMs). There are also patient satisfaction measures, which historically often have less to do with the clinical care than the hospital stay, such as the quality of the food. Patient-reported measures hold the most promise, with more investment recently in underpinning such measurements with scientific validation, like psychometrics. As Witkowski says, “If you ask one person who’s had a knee surgery, ‘How’s your pain?’ you have to ask yourself, ‘How does that subjective assessment relate to another person’s answer?’ There’s so much variability that physicians and clinical teams rightly feel like there’s too much noise.” Clinicians might measure mortality or range of motion, but it’s bigger than that. Measuring outcomes should be accessible and useful, says Witkowski. It should be grounded in patient care, useful to clinicians, and easily aligned with the technological solution used to track it.
Right now, the Centers for Medicaid & Medicare Services (CMS) and the National Quality Forum, among others, mandate that health facilities track metrics, but questions remain if they are the right ones and whether such measurements actually matter to the patient. Witkowski tells a hypothetical story to illustrate:
A doctor is going to remove a parotid tumor in your jaw. The neurosurgeon has to take that out without hitting the facial nerve. The current quality measures we have for that hospital typically don’t include how often the surgeon was able to get the complete tumor out without hitting the facial nerve. Rather, the surgeon is being measured on the hospital wide urinary tract infection rate. Nobody wants a urinary tract infection, but if I’ve got parotid cancer, do I care? And the difference between one hospital and another might hypothetically be an additional 0.05 percent chance of getting a urinary tract infection. But, as a patient, I would much rather go to the surgeon who has a 95 percent track record of not hitting the facial nerve versus somebody else who’s in the 70s, but their UTI rate is 0.05 percent lower.
Witkowski notes that time and time again she hears institutions say, “We already have so many measures. We’re overloaded from measures. So, we just want to put in a few that work across the hospital.” But if the few measures they are taking are meaningless, they become more of a burden. “As a physician,” Witkowski says, “I’d be much happier adding on 10 measures that really matter to my patients—that I feel is a good reflection of my work—than five measures that don’t pertain to me.”
Hope for the profession
The last year has caused us to think profoundly about the state of health care. “We know from COVID obviously that health is a global business,” says Witkowski. “If we have an infection that comes up in one part of the world, soon it’s going to be here. People suffer from diabetes the same way they do in Europe or Africa, as they do in the U.S. If we really want to do better, we’ve got to harness all that data.” In the U.S., health care innovation goes alongside health care costs. According to Witkowski, when CMS and Congress look to make any kind of changes to the health care system, “they say it has to cost less than the one before,” even if a greater investment in the short term may lead to better long-term outcomes.
Providers who are thinking differently, an awareness of inequity and social determinants of health, and an investment in electronic resources like telemedicine mean there is hope for the field, says Witkowski. The newest head of the National Quality Forum, Dana Safran, for instance, is focused more on invigorating new models and standards, while nonprofits like ICHOM are gaining in strength. CMS, which occupies 50 percent of the health care market, was previously focused on the process metric field and is now moving toward value-based payments (Witkowski’s research) and outcomes measurement with more interest. Clinical training is likewise attempting to reach medical students and health care practitioners. Witkowski and her colleagues teach the Essentials of the Profession course at Harvard Medical School (HMS). HMS, along with the Dell Medical School at the University of Texas at Austin, are two of the leaders in training clinicians to think contextually about the delivery system and long-term value for patients. Witkowski notes that they try to reach individuals at every step of their health care education—from residency to executive levels.
According to Witkowski, the standard in medicine needs to be long-term outcomes.
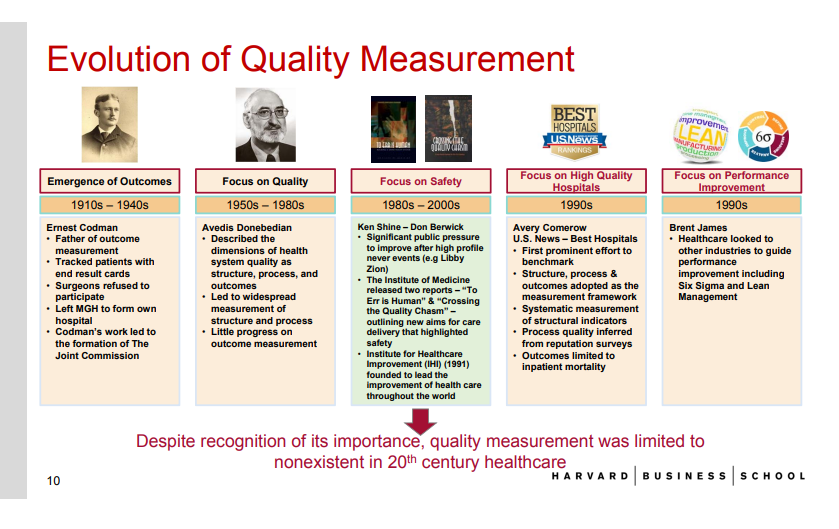
Health informatics is also a burgeoning field with a host of degree programs. Many schools offer undergraduate and master’s degrees in health informatics through their schools of information or public health. (This is not to be confused with biomedical or bioinformatics, which is a larger field with doctorate programs, though sometimes degree programs combine the disciplines.) The Commission on Accreditation for Health Informatics and Information Management Education (CAHIIM) has accredited 20 master’s programs in health informatics, including Boston University, the University of Michigan, and the University of Washington, and counts over 350 degree programs total. While outcomes measurement research in the clinical field has a long history going back to the early 20th century, medicine has only just begun to take it seriously (see figure 2 above). Educational institutionalization can help provide academic gravitas to the general idea that in health care, it is important to approach information technology and data carefully and rigorously.
According to Witkowski, the standard in medicine needs to be long-term outcomes. “If you build your business model around providing that long-term answer, it is the right thing to do. It’s the long game—I do think it would win—but people have a hard time focusing on the long game,” she says


