
In 1986 the Whitman-Walker Clinic, a medical practice focused on the needs of LGBTQ individuals in Washington, D.C., hired its first in-house lawyer to help “write wills, secure disability benefits, and fight discrimination” for a vulnerable patient population amid the HIV and AIDS crisis. In 1993 Dr. Barry Zuckerman at Boston Medical Center (BMC) hired a lawyer when he began noticing frustrating recurrent health issues in his pediatric patients that were caused and exacerbated by poverty; he realized seeking relief for his patients might require a legal strategy, not just a medical one. The Family Advocacy Project, as the BMC project became known, became a model for the future—the medical-legal partnership (MLP).
MLPs screen for “social determinants of health,” a term scholars use to describe how access to food, income, education, housing, and more can affect health outcomes. Today, there are more than 500 MLPs across the United States, operating either as academic partnerships with law school clinics and medical schools or as nonprofit collaborations with legal aid groups and health care providers in their service areas. These MLPs include, at a minimum, 37 children’s hospitals, 29 veterans’ affairs medical centers, 170 legal aid agencies, and 58 law schools, according to the most recent survey conducted by the National Center for Medical-Legal Partnership. Today, LegalHealth, a subsidiary of the New York Legal Assistance Group (NYLAG), is the largest MLP in the United States, serving more than 7,000 clients in partnership with roughly 38 medical facilities, from Mount Sinai Hospital to the Northport VA Medical Center. And new partnerships are popping up all the time: recently, a Harvard Law School graduate was awarded a prestigious Skadden Fellowship to help expand an existing partnership to veterans’ hospitals.
In their 2022 Justice Gap Report, the Legal Services Corporation estimates that “low-income Americans did not receive any or enough legal help for 92% of their civil legal problems.” One study analyzing Kaiser Permanente’s national MLP indicated that without Kaiser’s intervention, patients were likely to never have accessed legal help—because they either did not know their problems were legal in nature or had no way of getting a lawyer—and that “82 percent of cases were addressed with fewer than 5 hours of attorney time.” While housing remains the prototypical case in an MLP, in recent years, and in the wake of President Trump’s immigration crackdown, patients interacting with MLPs are increasingly also seeking immigration help. Broadly, MLPs offer a way to rethink how to serve people more holistically—a type of whole-person care.
Today, there are more than 500 MLPs across the United States, operating either as academic partnerships with law school clinics and medical schools or as nonprofit collaborations with legal aid groups and health care providers in their service areas.
But how do MLPs work to identify and address legal needs like immigration and food insecurity? And what does it mean to rethink how health care is delivered, how the access-to-justice crisis is eased, and how the medical and legal professions might better cross disciplinary boundaries? In this article, we talk to individuals involved in implementation and research around MLPs to understand how the field is moving the needle on health equity, as well as offering new models for professional collaboration.
“Our patients are their clients”
In 2017 the Legal Aid Society of Greater Cincinnati (LASGC) received a number of referrals for parents “struggling to add their newborn infants to their Supplemental Nutrition Assistance Program (SNAP) benefits,” a research team describes in a paper on the issue. Investigating why families kept running into trouble, the LASGC lawyers discovered an overly burdensome bureaucratic process—and with the county, they got to work dismantling it. Ultimately, the legal aid team’s persistence led to a streamlined system for enrollment in Medicaid-managed care more holistically. Many of the cases at LASGC for this particular problem came through their partnership with Cincinnati Children’s Hospital Medical Center.
“I can’t imagine doing this work without the lawyers,” says Dr. Andrew Beck, a primary care and hospitalist pediatrician at Cincinnati Children’s. Dr. Beck is also associate chief population health officer and director of research and innovation within the Office of Population Health and Michael Fisher Child Health Equity Center. “Our MLP enables doctors and lawyers to work together with a shared vision of supporting at-risk children and families,” says Adrienne Henize, Cincinnati Children’s program director of the MLP and lead for clinical-community partnerships in the Fisher Child Health Equity Center. “Our patients are their clients.”
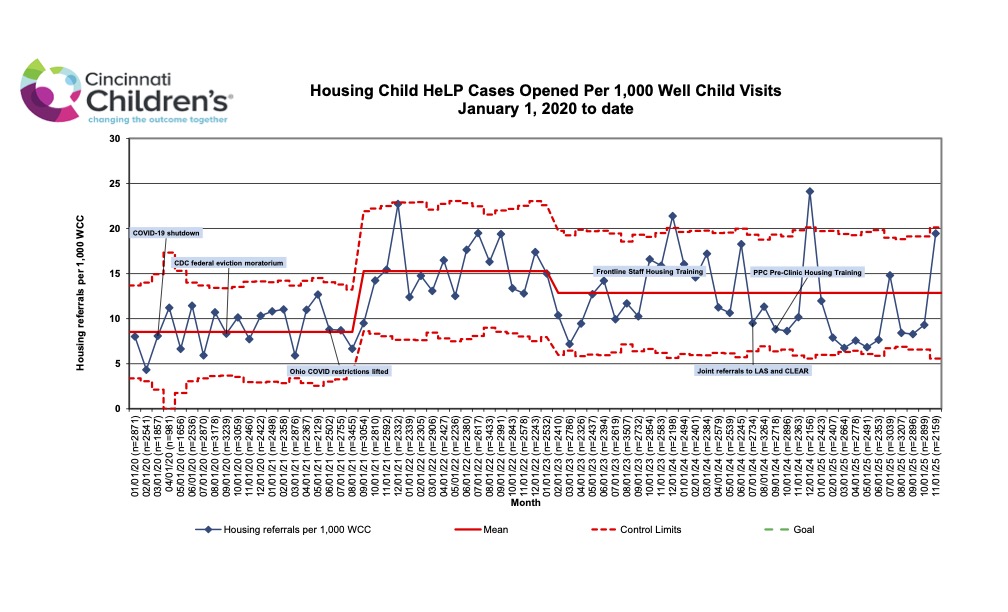
Since it launched in 2008, the Cincinnati Child Health-Law Partnership (Child HeLP) has worked with more than 24,000 children in referred households on cases related to housing, insurance, public benefits, education needs, and more, as well as recovered more than $2.2 million in back and adjusted future public benefits for families. Initial research from the collaboration also points to a reduction in hospitalizations for kids whose families received legal consultation. Though it’s difficult to pinpoint exactly why, researchers surmise that screening for social determinants of health and connecting families with lawyers can help avert crises and improve child health outcomes.
When Dr. Robert Kahn, now vice president of Health Equity Strategy, director of Fisher Child Health Equity Center, and professor of pediatrics, UC Department of Pediatrics, came together with Elaine Fink, former managing attorney of the Children and Education Practice Group at LASGC, to form Child HeLP, they started with primary care in the Division of General and Community Pediatrics. Today, that referral group has expanded as management of the partnership on the Cincinnati Children’s side has come under the Fisher Child Health Equity Center: LASGC attorneys now also receive clients from 11 subspecialities within Cincinnati Children’s, including from the sickle cell, diabetes, and adolescent medicine clinics, among others.
I consider myself a child health expert. I do not consider myself a housing expert. It makes a ton of sense for me to want to have a relationship with a housing expert I can turn to with questions or concerns.
Dr. Andrew Beck, primary care and hospitalist pediatrician, Cincinnati Children’s Hospital Medical Center
How does it work on the medical side? When patients come to the hospital or an affiliated community clinic, they complete a standardized social-needs screener codeveloped with LASGC. The screener asks patients about “food insecurity, benefits, housing, unmet educational needs, and more,” says Dr. Beck. But, crucially, “these are meant to be a conversation starter, not a conversation ender. Someone may say no to everything on that list, but then I may go into the visit and have a conversation, and a need or risk may still emerge,” he says.
After families have signed waivers for both the doctors and the lawyers to share information, referral orders are placed by medical team members within the electronic medical record. “It’s the same basic process as if I was referring to a pediatric cardiologist or a gastroenterologist,” says Dr. Beck. That generates an email to Henize, who then sends it to LASGC for intake and appropriate action.
Child HeLP tries to reduce barriers to the family obtaining legal help. The Pediatric Primary Care clinic has a legal advocate on-site at least two days a week who will try to see the referred family immediately. If the issue requires specialist attention or an advocate is not present, LASGC reaches out to the family within a few days.
Child HeLP has been a “model partnership” says Henize, whose team helps drive community collaboration for Cincinnati Children’s more generally to “ensure they are supporting kids in Greater Cincinnati who might not even come to the hospital.” Child HeLP has also led to other MLPs for LASGC, which launched M-HeLP, an MLP focused on maternal health in partnership with TriHealth, the largest birthing center in Cincinnati, and Cincinnati Children’s in 2017.
“Child HeLP has really helped us see the benefit of bringing in expertise that we might not have,” says Dr. Beck. “I consider myself a child health expert. I do not consider myself a housing expert,” he adds. “It makes a ton of sense for me to want to have a relationship with a housing expert I can turn to with questions or concerns.”
“A trusted relationship”
Each year, LASGC opens about 4,000 cases total. They receive about 1,000 to 1,200 referrals from Child HeLP and M-HeLP and open roughly 700 of them as cases. At the outset of the program, there was roughly an even split between cases focused on housing and income, and work and health (public benefits cases). Post-pandemic, housing issues spiked. Cincinnati’s housing stock is old, and there’s not enough of it, says Rachel Barr, senior attorney at LASGC who manages the MLP on the legal side. During COVID, doctors started seeing kids who were at home for more hours of the day, she guesses, and that time at home may have exacerbated any adverse health effects due to exposure to poor conditions.
After LASGC goes through a checklist to make sure families meet their income requirements, “as long as there is a legal issue to address and we don’t have a conflict, the case is then assigned to an advocate who is going to work it like they would work a case that comes through intake,” says Barr. But “the one unique part about working that case is we do have access to a doctor when we need them,” she adds. And the attorneys are not just talking to any doctor; they have access to the treating doctor. “That makes such a huge difference,” says Regina Campbell, managing attorney of the Income, Work, and Health practice group at LASGC, “especially in Social Security cases where courts are supposed to put more weight on the opinions of the people who see the child regularly and treat the medical condition that Social Security is reviewing.”
If I have a letter from the doctor that says, ‘This is the child’s condition, this is how it presents on a daily basis, and in my clinical opinion the incident at school is related to the disability,’ or even better, if I can have somebody from Children’s come with me to that meeting, it can make all the difference.
Rachel Barr, senior attorney, Legal Aid Society of Greater Cincinnati
Access to treating providers can also make a sizable impact in education cases, Barr says. If a child has a disability and the school has proposed expulsion for more than 10 days, they are required to do a manifestation determination review. “The school has to figure out if what the child did that led to the discipline incident is related to their disability, because if it is, they can’t remove the child from school—that would be disability discrimination,” she says. She explains further:
Lawyers go to those meetings all the time. Schools don’t look at us as the most neutral parties. I can make the argument that of course this incident is related to this child’s disability, but the school’s going to take that with a grain of salt. If I have a letter from the doctor that says, ‘This is the child’s condition, this is how it presents on a daily basis, and in my clinical opinion the incident at school is related to the disability,’ or even better, if I can have somebody from Children’s come with me to that meeting, it can make all the difference.
LASGC also works closely with the medical team to make sure they communicate more effectively with the legal system. For instance, approval of prior authorization in Medicaid cases requires showing that the treatment is medically necessary, which requires meeting several criteria. “We can try to teach health care providers how best to communicate a child’s needs to a managed care plan. By doing that, we are not only relying on the doctor’s expertise but helping craft how that expertise is articulated,” says Campbell.
Cross-clinical training
Barr and Campbell both regularly train health care providers about social determinants of health. This includes teaching in the pediatric advocacy rotation for medical residents. They see that as critical for system-level change, since residents could end up practicing anywhere after their training at Cincinnati Children’s. “By teaching providers about health-harming legal needs, they are able to better identify legal issues that a legal services organization might be able to help with. Even if you’re not here in Cincinnati, there should be a legal aid in whatever county they end up practicing in, so the training we provide is helping to connect folks in Cincinnati with legal services but also in other parts of the county as well,” Barr says.
Barr and Campbell have also done a lot of training with more senior physicians at Children’s, on both what makes a good referral and deep dives into areas of the law that might be helpful for them. There’s no reason medical staff would know what a legal issue looks like or what to do about it, so LASGC is filling in the gap to make sure their referral pool is as strong as possible. “We teach them how to issue spot. We want you to listen to that feeling in your gut when you hear somebody say, ‘My landlord did this really awful thing.’ You should listen to that, and you should refer them to us,” says Barr. The lawyers also train doctors in what lawyers can and cannot help with. “For example, unfortunately, in Ohio, there’s not a whole lot you can do about bullying from the legal perspective,” she adds.
The perspectives complement each other, says Campbell. “Doctors think, ‘This health system isn’t good for kids, period.’ And then our role is to say, Don’t put a period—put a comma and what are we going to do about it?” she says.
“We’ve focused a lot of attention over the years on building and sustaining a trusted relationship between our team on the medical side and their team on the legal side, and we’ve done it in a way that I think has really enabled the partnership to remain strong and to grow,” says Dr. Beck. As the lawyers invested in their training and relationship with psychiatry, for instance, they started to hear about a complicated pattern of cases that could benefit from system-level thinking. Like many legal aid groups, LASGC aims to do about 50 percent impact work along with 50 percent direct representation. A number of children who were in inpatient psychiatric care were ready to be discharged, Barr says, but they could not yet go home.
“They still need a lot of treatment, they need a lot of structure, they need a lot of support, and oftentimes they’re still a danger to the people in their household,” says Barr. Right now, the “step-down” options are few and far between. The waiting list for the beds covered by Medicaid is long, and the options not covered are “through an alternative funding structure that doesn’t offer you due process rights if you’re denied,” says Barr. Over the past year, a team of four attorneys has been researching the system and identifying cases in an attempt to change the system. “We knew there was probably a problem there, but we couldn’t really put our finger on what the problem was until those cases emerged and until we were able to develop that team,” says Barr.
Doctors think, ‘This health system isn’t good for kids, period.’ And then our role is to say, Don’t put a period—put a comma and what are we going to do about it?
Regina Campbell, managing attorney, Income, Work, and Health practice group, LASGC
Campbell and Barr both feel they have started to see more impactful results as they continue to work closely with doctors, even when there’s tension, like when they realized the legal world and the medical world have different definitions of “quick,” says Campbell. They share and celebrate success stories across the team, which meets monthly as a whole group and is in contact daily. “Child HeLP enables each of our professions to do more than we would be able to do if we weren’t working together,” says Henize.
“Learning while their professional identity is being formed”
As clinical faculty at Georgetown Law Center, Yael Zakai Cannon and her collaborators realized that the medical school and law school at Georgetown “were both working deeply in underserved communities in Washington, D.C., but doing so separately.” Georgetown Medical School’s motto is “cura personalis,” or “treat the whole person,” and they already a KIDS mobile medical clinic designed to provide low-barrier care in communities underserved by the health care system. What would happen if they integrated law students into that mobile clinic? In 2016 Georgetown’s Health Justice Alliance was born, an academic MLP that thoughtfully pairs students between schools to work with community members across DC to address social determinants of health.
According to scholarship from Georgetown and the National Center for Medical-Legal Partnership, “an academic MLP (A-MLP) [is] a specific type of MLP with three motivating goals: 1) educating pre-professional learners, 2) intentionally creating interprofessional learning environments, and 3) contributing to the evidence base for the MLP model as a health equity intervention.” Cannon believes deeply in the model as an innovative approach to professional training. “Both med students and law students gain valuable skills from learning to collaborate while their professional identity is being formed,” says Cannon. That is, before professional silos are engrained.
Today, law students partner with medical students to serve patients of the KIDS mobile medical clinic in an immersive experiential learning semester. Law students enroll in the Health Justice Alliance’s Law Clinic, which Cannon directs, as a 10-credit course. They usually take only one or two other classes on the side. Medical students working with the Law Clinic do so as a full-time rotation during their fourth year of schooling for one or two months. They partner closely with the law students to advocate for patient families. Medical students also join the law students in the classroom to learn about the role of law in driving health inequity and to develop advocacy skills.
“We have law and medical students literally sitting around a table throughout the day, trying to holistically think through the problems our clients are facing and how they can bring their various tools together,” says Cannon. In medical education, especially, Cannon says this is novel. “Many medical schools across the country have a deep curriculum around the social determinants of health,” she says. “What our students experience is different—our medical students are with our law students in a family’s home, talking with them, and seeing with their own eyes how these drivers of health are harming families who have been marginalized.”
Law students likewise learn how to shift their perspective—“to be a holistic client-centered thinker” and not simply think of problems as “legal in nature,” says Cannon. This is crucial for the practice of law more broadly, she says, as a student may be asked to master a variety of other disciplines across a legal career. In the seminar room, medical students are able to share their perspectives, like best practices for patient interviewing, with law students, who can then bring that expertise to their own client interviews.
When kids come into the mobile clinic, they receive a tablet with a “well-being screening,” a “tool that we designed with our medical partners and with feedback from our patient families that asks about a number of issues that serve as social and structural barriers of health,” says Cannon. The pediatric team is deeply trained to then ask follow-up questions and, if applicable, refer the family to the law students.
We have law and medical students literally sitting around a table throughout the day, trying to holistically think through the problems our clients are facing and how they can bring their various tools together.
Yael Zakai Cannon, professor of law, Georgetown University Law Center
Crucially, the referral is not a hand-off—it’s integrated care. Medical providers continue to work with law students as they proceed on their cases. For instance, Cannon’s team was working with a number of doctors who were seeing case after case of asthma. “Asthma should never be fatal for children. But it can be in D.C.,” says Cannon, given a range of health risks such as long-standing issues around substandard housing.
Cannon’s students recently worked closely with a family where the child had asthma and the parent had cancer. A nearby construction project had caused a rodent infestation, particularly dangerous to a family with multiple immunocompromised members. The law students and the medical students traveled to the family to interview them together. In a situation like this, the team might retain an extermination expert or interview other neighbors. But they had more than that: “What’s remarkable is the research that our medical students do to help us understand, What is the type of cancer that this parent has, what is the treatment they’re undergoing, and what does the medical literature say about how a mice infestation can impact this family’s health?” Cannon explains. “With that literature in our hand, we have so many more legal avenues open to us.” They could explore disability rights law and reasonable accommodations or a temporary restraining order to get emergency relief or rent abatement. Cutting back on her work hours and struggling with her finances, the parent was also being threatened with eviction. “If a mom with cancer and a child with asthma end up unhoused, all of the medical literature says there are horrible outcomes that this family is at risk for, including early mortality,” Cannon says.
The team was able to not only get the infestation remediated and prevent the eviction, they were able to think broadly about how to address the parent’s other concerns. They helped her understand her right to Social Security disability benefits and helped her apply for them, and they helped her obtain medical leave, food assistance, childcare assistance, and more. “This type of really holistic advocacy is only possible because our students are in a really immersive experience and they are collaborating across professions,” says Cannon.
Today, the Health Justice Alliance comprises three different opportunities for law students beyond the initial pediatric focus: Cancer LAW, Perinatal LAW, and a medical-financial law focus. The Cancer LAW project sprang up because the Health Justice Alliance legal team began hearing from “oncologists who were saying, ‘Wow, we have a lot of patients missing really critical lifesaving treatment appointments. And when we talk to them about it, they say something like, ‘Cancer is number 10 on my list of problems,’” Cannon reports. If you’re late on rent payments and getting evicted or have trouble getting childcare, seeking cancer treatment might fall by the wayside. The focus on perinatal law aims to reduce grave disparities in maternal and infant mortality among underserved communities in D.C., and the medical-financial focus means law students are now in the mobile clinic doing a “public benefits checkup” with patients. The intentional expansion of the MLP ultimately points to the success of both the training experience for med and law students as well as better outcomes for the population they serve.
An innovation in access to justice
The opportunity to provide legal help in a doctor’s office—a place of trust—is critical, says Cannon. “A lot of people think of the MLP as a revolution in health care, and it is. But it’s also a complete innovation in how we approach access to justice.” Most people seek out a lawyer only when they are in “crisis”—they’re facing eviction, and they are suddenly wading through bureaucracy to find out what level of help is available to them. Connecting individuals with a lawyer through a doctor’s visit is just removing one more barrier; they may not have even realized the issue they were dealing with has a legal remedy, Cannon points out. It is a “low-barrier model” when there are already so many barriers to individuals accessing justice.
Cannon writes about this in more detail in a piece for Stanford Law Review, explaining that legal aid agencies are often thought of as emergency rooms for legal needs. MLPs “offer a model that is community-integrated, preventive, interdisciplinary, and transformative,” she writes. To further expand such low-barrier access to justice, Cannon asks, legal services could be integrated into more than just doctor’s offices: What about libraries, schools, nursing homes, and churches?
A lot of people think of the MLP as a revolution in health care, and it is. But it’s also a complete innovation in how we approach access to justice.
Yael Zakai Cannon
Bethany Hamilton, director of the National Center for Medical-Legal Partnership (NCMLP) at the George Washington University Milken Institute School of Public Health, views MLP as an ideal setting for developing transdisciplinary models of care. “When you think about what MLPs have already demonstrated—the ability to work beyond silos through multidisciplinary and interdisciplinary activities—it becomes clear that the field has the foundations for creating something even more integrated,” she says.
The MLP field is working to address an enduring challenge common to social interventions: overcoming barriers to sustainability and scale. “This is not just about severe underfunding but also about the structural choices that shape the field and practice. We must push ourselves to reimagine the very concepts of ‘integration’ and ‘linkage,’” says Hamilton. She adds that while a fully integrated clinic might include lawyers, social workers, and community justice practitioners, true integration requires more than colocation. “Everything from the physical space to the software, the staffing, and the decisions about care or representation are informed by and designed to support a completely unified framework—one that facilitates universal access and respects all stakeholders, especially the patients, as agents of justice.
But all of this could be tenuously held together if one crucial part is lost—the L in MLP.
“This transformation cannot start or end in the clinic,” she adds. “It requires that we set our intentions on ensuring that we do not rebuild the very silos we are trying to dismantle.” As evidence of the field’s transformation, Hamilton highlights how MLPs have evolved to address more than civil legal needs. “A decade ago, I was told the MLP field was not ready to consider criminal legal needs as part of the model,” she says. While the traditional MLP still focuses on addressing civil legal needs that affect health outcomes, she says, “now, there are high-performing, research-driven MLPs that incorporate criminal legal needs as well.”
But all of this could be tenuously held together if one crucial part is lost—the L in MLP. The Legal Services Corporation provides the bulk of funding to legal aid organizations in the U.S. For 2026, Congress appropriated $540 million for that support. Hamilton considers this a partial win, as it still a reduction to an already underfunded agency that has consistently demonstrated need and impact, she says. Unmet social and legal needs will inevitably surface in health care settings. The MLP approach provides one pathway to address and prevent a broader systemic crisis. But, she argues, that can only happen if ample and stable funding remains in place.


